
AKI (Acute Kidney Injury) : DEFINITION, CLASSIFICATION AND CAUSES
AKI :
Rapid decrease in the kidney’s ability to eliminate waste products such as urea and creatinine. Other manifestations include decreased urine output, metabolic acidosis and hyperkalemia.
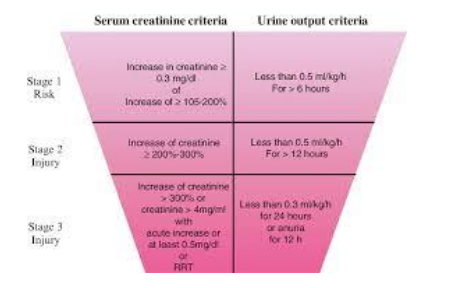
It can be defined and classified using changes in s. creatinine levels and urine output using the RIFLE criteria. This divides AKI into categories of RISK, INJURY, FAILURE, LOSS and END STAGE KIDNEY DISEASE.
CLINICAL CLASSIFICATION
Prerenal Renal (Parenchymal or Intrinsic) Postrenal
PRERENAL RENAL FAILURE:
Initial stage. It is functional in nature. Kidneys malfunction because of systemic factors that decreases GFR (decreased cardiac output, hypotension, sepsis etc.)
If the systemic cause is removed , renal function improves and relatively rapidly returns to normal levels.
If intervention is delayed or unsuccessful, renal injury becomes established (structural) and several days or weeks are required for recovery.
PARENCHYMAL RENAL FAILURE:
Principal source of damage is within the kidneys and structural changes can be seen in microscopy.
Causes of parenchymal AKI : GLOMURELONEPHRITIS
- VASCULITIS
- INTERSTITIAL NEPHRITIS
- MALIGNANT HYPERTENSION
- PYELONEPHRITIS
- BILATERAL CORTICAL NECROSIS
- AMYLOIDOSIS
- MALIGNANCY
- NEPHROTOXINS
- CHOLESTROL EMBOLISM
- Removal of nephrotoxins rapidly improves AKI.
Most common type of intrinsic AKI falls under ACUTE TUBULAR NECROSIS. It is assumed that tubular necrosis results from continuous hypoperfusion.
HEPATORENAL SYNDROME:
This form of AKI develops in severe liver dysfunction in the absence of other known causes of ARF. It presents as progressive oliguria with a very low sodium concentration (
Newer concensus defines HRS as any development of AKI in the setting of advanced liver disease that is not due to intrinsic causes.
RHABDOMYOLYSIS:
Pathogenesis includes prerenal, renal, postrenal factors. It is seen following major trauma , drug overdose, vascular embolism and in response to various agents that can induce major muscle injury.
Treatment include prompt and aggressive fluid resuscitation, elimination of causative agent, correction of compartment syndromes, alkalinisation of urine (pH>6.5) and the maintenance of polyuria (>300 ml/h).
POSTRENAL RENAL FAILURE:
Obstruction to urine outflow is the most common cause of functional renal impairment in the community but uncommon in the ICU. However sudden and unexpected anuria in ICU patients should always suggest obstruction of urinary catheter.
DRUGS CAUSING AKI IN ICU
- RADIOCONTRAST AGENTS
- AMINOGLYCOSIDES
- AMPHOTERICIN
- NSAIDS
- BETA LACTUM ANTIBIOTICS
- SULFONAMIDES
- ACYCLOVIR
- METHOTROXATE
- CISPLATIN
- CYCLOSPORIN A
- TACROLIMUS
- SIROLIMUS
- STARCH SOLUTIONS
RESULTS AND DISCUSSIONS:
AKI is a common occurrence in ICU. In this study of 200 patients being admitted to Medical ICU it was found that 94% of them were admitted with AKI. Around 6% developed AKI in ICU causes ranging from drugs to hypovolemia.
Of these 200 patients 78% were males and 22% females.
Age wise distribution showed an incidence of 46% in the elderly group of age more than 65, 35% in age group 45-60, 16% in 30-45 and 3% in 15-30 years of age. In the younger population GN was found to be the most common cause.
79% of these patients had a known CKD background whereas 21% were found to have AKI on non CKD.
Sepsis was found to be the most common cause having an incidence of around 56%. Heart failure was found to have an incidence of 16% followed by ACS with 13% occurrence. Other causes include HRS and GN with 4%, hypovolemia 3%, drugs with 2% and DKA and Snake bite with 1% each.
Hemodialysis was done for 33% of these patients and 67% were managed without any RRT.
61% of these patients were discharged from ICU and 17% opted for self-discharge (LAMA). The mortality in these 200 patients was found to be around 26%.
Of the total number of deaths 45% underwent hemodialysis and 55% were managed without RRT.
The percentage of patients developing AKI after admission was found to be 6%. The mortality rate in this group was 33% of whom all the patients had dialysis.
CONCLUSIONS:
AKI has been found in early 20th century medical literatures being described as War Nephritis. Despite of such early recognition research has been not extensive due to contrasting and contradictory definitions.
This changed with the introduction of the RIFLE criteria for AKI in 2004 by the Acute Dialysis Quality Initiative (ADQI). This defined AKI with changes in the S. CREATININE levels and urine output of the patient. Now RIFLE criteria is widely used in ICUs to assess AKI. The incidence of AKI has been on a rise probably due to better detection and recognition. Still it is one of the most under reported entities in the ICU. Mortality in ICU was about 26% and patients developing AKI after admission had a greater mortality rate although dialysis was done for these patients. The study was limited by the total number of patients who developed AKI post admission. Further study is required to identify those patients developing AKI in ICU, mortality in these patients and modifiable risk factors.
REFERENCES:
- Mehta RL, Kellum JA, Shah SV, et al. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Critical Care. 2007;11, article R31
- Ostermann M, Chang RWS. Acute kidney injury in the intensive care unit according to RIFLE. Critical Care Medicine. 2007;35(8):1837–1843
- Hoste EAJ, Clermont G, Kersten A, et al. RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis. Critical Care. 2006;10
Author:
DR. Manash Ranjan Chaudhury
Fellow, Critical care Medicine
Narayana Superspeciality Hospital
Guwahati, Assam




Customer Reviews
Thanks for submitting your comment!